9008
PreStride4®
The PreStride4®, model 9008 is the same as model 9007, except it utilizes our new Stride4® (Patent Pending) stance control knee joints. The Stride4® is comprised of a four bar linkage mechanism that offers three modes of operation: Stance control, free motion, and locked with stance phase flexion. An integral extension assist spring housed within the midsection assists with knee extension, while an adjustable extension stop allows the practitioner to adjust and fine tune the point at which the joint enters into its stable/locked state. A button on the Stride4® knee joint allows the practitioner to switch between stance control and locked modes of operation. When the lock option is selected and engaged by the clinician, the joint will allow approximately 3° of flexion to provide some shock absorption to the patient. An additional advantage of the PreStride4® is that it may be used as an effective gait training tool during rehabilitation.
For more and information please visit our product spotlight page.
Knee Joint Selection Guide
 Downloadable Version
Downloadable Version
Discretion in choosing a joint size and designing an appropriate orthosis should be used by the orthotist in all cases. We would reference and support the approach described by Lunsford and agree that successful orthotic management requires a clear understanding of the condition being treated and a realistic plan to address the biomechanical deficits presented.
For optimal orthotic management, the mechicanical demands to be placed upon the orthosis for any given treatment must be understood prior to material selection.
The selection of the correct materials is often the difference between success and failure and we believe that the orthotist is trained and the best qualified to match the characteristics of the material to the biomechanical and functional needs of the patient.
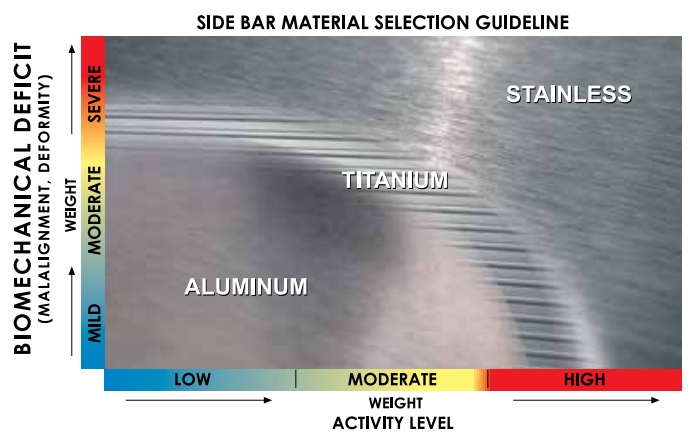
Discretion in choosing a joint size, selecting the Side Bar Material, and designing an appropriate orthosis should be used by the orthotist in all cases. The following factors are commonly used by orthotists to help determine the level of Biomechanical Deficit. Practical issues including compliance, occupation, environment and social factors should also be taken into consideration.
Biomechanical Deficit Factors
- Single or multiple plane involvement
- Single or multiple segment involvement
- Muscle strength/weakness
- Range-of-motion
- Skeletal and/or joint alignment — malalignment
- Mobile or fixed deformity
- Presence and magnitude of joint contracture
- Presence/extent of spasticity
- Proprioceptive and cognitive skills
- Progressive or non progressive condition
| Biomechanical Deficit | Mild | Moderate | Severe | |||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Activity Level | Low | Moderate | High | Low | Moderate | High | Low | Moderate | High | |||||||||||||||||||
|
Patients Weight LBS (kg) |
80-140 (36-64) |
140-210 (64-95) |
210-320 (95-145) |
80-140 (36-64) |
140-210 (64-95) |
210-320 (95-145) |
80-140 (36-64) |
140-210 (64-95) |
210-320 (95-145) |
80-140 (36-64) |
140-210 (64-95) |
210-320 (95-145) |
80-140 (36-64) |
140-210 (64-95) |
210-320 (95-145) |
80-140 (36-64) |
140-210 (64-95) |
210-320 (95-145) |
80-140 (36-64) |
140-210 (64-95) |
210-320 (95-145) |
80-140 (36-64) |
140-210 (64-95) |
210-320 (95-145) |
80-140 (36-64) |
140-210 (64-95) |
210-320 (95-145) |
|
| 1001 | B | A | — | B | A | — | B/A | A | — | B | A | — | B | A | — | B/A | A | — | B/A | A | A | B/A | A | — | B/A | A | — | |
| 1002 | B | A | — | B | A | — | B/A | A | — | B | A | — | B | A | — | B/A | A | — | B/A | A | A** | B/A | A | A** | B/A | A** | — | |
| 1003 | B | A | — | B | A | — | B/A | A | — | B | A | — | B | A | — | B/A | A | — | B/A | A | — | A | — | — | A | — | — | |
| 1004 | B | A | — | B | A | — | B/A | A | — | B | A | — | B | A | — | B/A | A | — | B/A | A | — | A | A | — | A | — | — | |
| 1006* | B | A | — | B | A | — | B/A | A | — | B | A | — | B | A | — | B/A | A | — | B/A | A | — | A | A | — | — | — | — | |
| 1007* | B | A | — | B | A | — | B/A | A | — | B | A | — | B | A | — | B/A | A | — | B/A | A | — | A | — | — | — | — | — | |
| 1010* | B | A | — | B | A | — | B/A | A | — | B | A | — | B | A | — | B/A | A | — | B/A | A | — | A | — | — | — | — | — | |
| 1012 | B | A | — | B | A | — | B/A | A | — | B | A | — | B | A | — | B/A | A | — | B/A | A | — | B/A | A | — | — | — | — | |
| 1013* | — | A | — | — | A | — | A | A | — | — | A | — | — | A | — | A | A | — | A | A | — | A | — | — | — | — | — | |
| 1015 | B | A | — | B | A | — | B/A | A | — | B | A | — | B | A | — | B/A | A | — | B/A | A | A | A | A | — | — | — | — | |
| 1017 | B | A | — | B | A | — | B/A | A | — | B | A | — | B | A | — | B/A | A | — | B/A | A | — | B/A | A | — | A | A | — | |
| 1017-A38* | — | — | A | — | — | A | — | — | A | — | — | A | — | — | A | — | — | A | A | A | A | A | A | A | A | A | A | |
| 2004* | B | B | — | B | B | — | — | — | — | B | B | — | B | B | — | — | — | — | B | — | — | — | — | — | — | — | — | |
| 2009* | B | A | — | B | A | — | B/A | A | — | B | A | — | B | A | — | B/A | A | — | B/A | A | — | A | A | — | A | — | — | |
| S2001* | B | A | — | B | A | — | B/A | A | — | B | A | — | B | A | — | B/A | A | — | B/A | A | — | A | A | — | A | — | — | |
| S2003* | B | A | — | B | A | — | B/A | A | — | B | A | — | B | A | — | B/A | A | — | B/A | A | — | A | A | — | A | — | — | |
- * Not available with titanium uprights.
- ** Consider ordering with Heavy Duty Rings, Model 1002-A#4HD.
- NOTE: Model 1017-A38 is available with aluminum uprights only.
Steel and Aluminum Alloys
Steel is stronger and stiffer than aluminum allow; aluminum allow has a lower density making it lighter. Steel is fatigure resistant and combines high rigidity, or ductility depending on the alloy. The main disadvantage of steel is its weight. The major benefit of aluminum in orthotics is its high strength to weight ratio. Aluminum does however have a lower endurance limit under repreated dynamic loading conditions than does steel. A common clinical question relates to the upright of a lower extremity orthosis in which deformation under bending stresses is very important. In general terms, if loading conditions are known to be great or highly repetitive, steel is superior to aluminum.
Considerations for preventing failure:
- Fatigue
- Stress Concentration
- Finishing
- Bend Radii
- Design